12. What Positions May the Baby Be Placed in to Facilitate Drainage of the Respiratory Tract?
Introduction [edit | edit source]
The term chest physiotherapy (CPT) stands for a spectrum of physical and mechanical interventions aimed at interacting therapeutically with astute and chronic respiratory disorders.[1]Amidst diverse techniques for airway clearance, postural drainage is ane of the widely used methods since decades.
Definition [edit | edit source]
Postural drainage is the positioning of a patient with an involved lung segment such that gravity has a maximal consequence of facilitating the drainage of broncho-pulmonary secretions from the tracheobronchial tree.[2]It is based on the concept of gravity-assisted mobilization of secretions and transport it for removal. It is a positioning technique to mobilize bronchial secretions.
Mechanism [edit | edit source]
During erect position simply the segments of the right upper lobe and non-lingular portion of the left upper lobe receive gravitational help whereas the segment of the middle, lingular portion of left upper lobe and lower lobe segments of both lungs must drain against gravity. In normal healthy land, the mucociliary machinery clears off the bronchial secretions. In diseased state they get compromised and secretions get accumulated specially in the smaller airways that cannot be emptied without gravity aid which tin further lead to inflammation and scarring.[3]The natural methods of elimination the tracheo-bronchial tree of accumulated secretion are on the whole extremely inefficient. Ciliary action -only removes infinitesimal particulate thing such equally dust or leaner, and is of no value when there is much secretion.[iv]
Procedure [edit | edit source]
The patient is tilted or propped at an bending required and chest percussion is performed to loosen the secretions. Frames, tilt tables, and pillows may be used to back up patients in these positions.[one] At that place are postural beds that have a hinge in the middle.
In full general, the upper lobe segments have the advantage of gravity drainage both in cock as well equally in semi recumbent position, so postural drainage can be facilitated in sitting or lying posture. The middle and lower lobes exercise not have the advantage of gravity drainage in erect, semi-recumbent or recumbent postures.
A foot end elevation of 14-18 inches is requires for the drainage of middle and lower lobes.[3] Each position consists of placing the target lung segment(s) superior to the carina. Positions should generally be held for 3 to xv minutes (longer in special situations). Standard positions are modified as the patient'south status and tolerance warrant.
In disquisitional care patients, including those on mechanical ventilation, Postural Drainage should be performed from every 4 to every 6 hours every bit indicated. PDT lodge should be re-evaluated at least every 48 hours based on assessments from private treatments. Domiciliary patients should be reevaluated every iii months and with alter of status.[5] . In the actively cooperating patient, postural drainage can be complemented by thoracic expansion exercises and by breathing command.[one]
Positions [edit | edit source]
Upper Lobe [edit | edit source]
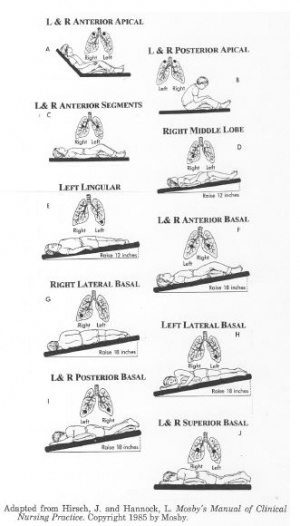
APICAL SEGMENTS -The patient should sit down upright, with slight variations according to the position of the lesion which may necessitate leaning slightly j backward, forward or sideways. The position is usually only necessary for infants or patients beingness nursed in a recumbent j position, but occasionally may be required if at that place is an abscess or stenosis of a bronchus in the apical region.
Inductive SEGMENTS - The patient should lie flat on his dorsum with his arms relaxed to his side; the knees should be slightly flexed over a pillow.
POSTERIOR SEGMENT
- Correct - The patient should lie on his left side then plough 450 on to his face, resting against a pillow with some other supporting his head. He r should place his left arm comfortably behind his dorsum with his correct arm resting on the supporting pillow; the right knee should exist flexed.
- Left - The patient should lie on his correct side turned 450 on to his face with three pillows arranged to raise the shoulder 30cm (i2in) from the bed. He should place his correct arm behind his dorsum with his left arm resting on the supporting pillows; both the knees should be slightly bent.
Middle Lobe [edit | edit source]
LATERAL SEGMENT: MEDIAL SEGMENT The patient should lie on his dorsum with his torso quarter turned to the left maintained by a pillow under the correct side from shoulder to hip and the arms relaxed by his side; the human foot of the bed should be raised 35cm (14in) from the ground. The chest is tilted to an angle of 15°.
Lingula [edit | edit source]
SUPERIOR SEGMENT: Inferior SEGMENT - The patient should lie on his back with his trunk quarter turned to the right maintained by a pillow under the left side from shoulder to hip and the arms relaxed by his side; the foot of the bed should be raised 35cm (14m) from the ground. The chest is tilted to an bending of 15°.
Lower Lobe [edit | edit source]
Apical SEGMENTS - The patient should lie prone with the head turned to i side, his arms relaxed in a comfortable position by the side of the caput and a pillow under his hips.
Anterior BASAL SEGMENTS - The patient should lie flat on his back with the buttocks resting on a pillow and the knees aptitude; the foot of the bed should exist raised 46cm (i8in) from the basis. The chest is tilted to an angle of 20°
POSTERIOR BASAL SEGMENTS - The patient should lie prone with his head turned to 1 side, his arms in a comfortable position past the side of the head and a pillow nether his hips. The foot of the bed should exist raised 46cm (i8in) from the ground. The breast is tilted to an angle of xx°.
MEDIAL BASAL (CARDIAC) SEGMENT - The patient should lie on his right side with a pillow under the hips and the foot of the bed should exist raised 46cm (i8in) from the footing. The chest is tilted to an angle of twenty°.
LATERAL BASAL SEGMENT - The patient should prevarication on the opposite side with a pillow under the hips and the human foot of the bed should be raised 46cm (i8in) from the ground. The chest is tilted to an bending of twenty°.
Assessment [edit | edit source]
The following should exist assessed and reported to establish a need for postural drainage[v]:-
- A contempo radiograph or bronchogram if bachelor, is a useful adjunct in isolating the afflicted areas.
- Pulmonary Office Test
- excessive sputum production
- effectiveness of cough
- history of pulmonary problems treated successfully with PDT (e.k., bronchiectasis, cystic fibrosis, Lung Abscess)
- decreased breath sounds or crackles or rhonchi suggesting secretions in the airway
- change in vital signs
- Aberrant chest x-ray consistent with atelectasis, mucus plugging, or infiltrates
- deterioration in arterial blood gas values or oxygen saturation
Indications [edit | edit source]
The post-obit are the indications for postural drainage[5]:-
- evidence or suggestion of difficulty with secretion clearance
- difficulty clearing secretions with expectorated sputum product greater than 25-30 mL/twenty-four hours (adult)
- evidence or suggestion of retained secretions in the presence of an artificial airway
- presence of atelectasis caused by or suspected of beingness caused by mucus plugging
- diagnosis of diseases such as cystic fibrosis, bronchiectasis or cavitating lung disease
- presence of foreign torso in airway
Contraindications [edit | edit source]
The post-obit are contraindications for postural drainage[6]
- often non suitable for infants in the NICU, who may have lots of equipment attached to them[7].
- Head injuries including cognitive vascular accidents because intracranial pressure level would be increased.
- Severe hypertension every bit venous render is increased with tipping and this can overload the heart.
- Following esophagectomy in that location tin can be undue stress on the anastomosis and tipping may crusade regurgitation.
- Severe hemoptysis, when all forms of physiotherapy should exist discontinued until there has been give-and-take with the doctors.
- Aortic aneurysms which would be put nether tension if the patient is tipped.
- Pulmonary edema which collects in the dependent areas; postural drainage would cause extreme dyspnea and probably worsen the state of affairs.
- Surgical emphysema which might rails toward the face if the patient is tipped and might result in dyspnea. Tension pneumothorax without an intercostal drain. This condition should not require physiotherapy, but must never exist tipped as the cardiac embarrassment may lead to a cardiac abort.
- Cardiac arrhythmias which can be worsened by postural bleed-ane historic period; in some positions the myocardial oxygen demand would be greater and so its sensitivity to abnormal rhythms is increased
- Hiatus hernias should not be tipped as the patient may regurgitate gastric juices.
- The filling cycle of peritoneal dialysis. The descent of the diaphragm is impeded during this phase and tipping may cause more respiratory distress.
- Facial edema from burns will be increased with tipping
- Eye operations where at that place may be some associated edema which could be increased with tipping.
- ↑ 1.0 1.ane 1.two Zach, Grand. Southward., & Oberwaldner, B. (2008). Chest Physiotherapy. Pediatric Respiratory Medicine, 241–251. doi:x.1016/b978-032304048-8.50022-0
- ↑ West MP. Postural Drainage. Acute Care Handbook for Physical Therapists. 2013 Sep 27:467.
- ↑ 3.0 3.1 Balachandran A, Shivbalan Due south, Thangavelu S. Chest physiotherapy in pediatric practice. Indian pediatrics. 2005 Jun 1;42(6):559.
- ↑ Nelson HP. Postural drainage of the lungs. British medical journal. 1934 Aug eleven;two(3840):251.
- ↑ 5.0 5.1 5.2 Sobush DC. The development of a clinical practice guideline: from breast physical therapy (CPT) to postural drainage therapy (PDT). Cardiopulmonary Physical Therapy Journal. 1992 Oct ane;3(3):4-7.
- ↑ Downie PA, Innocenti DM, Jackson SE. Cash'due south textbook of chest, heart and vascular disorders for physiotherapists.
- ↑ Goldsmith JP, Karotkin Due east, Suresh Chiliad, Keszler M. Assisted ventilation of the neonate E-book. Elsevier Health Sciences; 2016 Sep 2.
Source: https://www.physio-pedia.com/Postural_Drainage
0 Response to "12. What Positions May the Baby Be Placed in to Facilitate Drainage of the Respiratory Tract?"
Post a Comment